


Introduction
Penile shaft skin loss represents a severe and functionally significant condition that may result from various causes, including mechanical trauma (e.g., machinery-related injuries), burns, necrotizing infections, postoperative complications of circumcision, or the injection of foreign materials into the penis. In some cases, it may also occur secondary to chronic conditions such as diabetes mellitus or peripheral vascular disease. Skin grafting has been applied as a clinical method for wound coverage since Reverdin first introduced the skin grafting technique in 1869¹. Diabetes mellitus delays wound healing and increases the risk of surgical site infections².
Autologous skin grafting is an effective technique for managing skin defects resulting from trauma, infection or inflammation, surgery, or oncologic treatment. The scalp is considered a particularly advantageous donor site, as it can provide repeated harvests without permanent loss of hair follicles. Scalp skin offers a large surface area, rapid healing, favorable aesthetic results, and the potential for hair regrowth even after multiple harvests from the same site 3,4,5.
Penile skin deficiency—whether caused by trauma, infection, burns, or congenital anomalies—can lead to penile shortening, curvature, painful erection, dysuria, and recurrent infections. These deformities not only affect the aesthetic appearance but also contribute to psychological distress, sexual dysfunction, and diminished quality of life. Without timely reconstruction, fibrosis, penile contracture, and erectile dysfunction may develop. Therefore, managing genital skin defects in patients with diabetes mellitus poses a significant challenge for both reconstructive and endocrine surgery.
Herein, we report a successful surgical case of penile shaft skin reconstruction using a split-thickness scalp skin graft in a diabetic patient with extensive penile skin loss secondary to diabetic complications.

Figure 1. Preoperative appearance of the patient’s scrotal region.
A 59-year-old male patient with a 6-year history of type II diabetes mellitus presented with poorly controlled blood glucose levels and an unclear treatment regimen. Approximately three weeks prior to admission, the patient developed an abscess and extensive cellulitis involving the lower abdominal wall and genital area, accompanied by swelling and ulceration. Subsequently, purulent discharge appeared at the ulcer site, followed by urinary retention. The patient underwent debridement and abdominal flap coverage at a local facility before being transferred to the National Hospital of Endocrinology for further management of diabetes and surgical reconstruction of penile skin loss.
On admission, the patient was alert, oriented, and thin in body habitus. The abdominal wound measured approximately 30 cm in length, with delayed healing, while the penile shaft exhibited complete loss of skin and persistent serous exudate through the dressing. Laboratory findings were as follows: capillary glucose 20.6 mmol/L; blood biochemistry showed urea/creatinine 18.9/111; AST/ALT 102/102; and C-reactive protein (CRP) 33.41 mg/L.
A detailed history revealed that the penile skin loss had occurred about three weeks before admission, beginning with pruritus and scratching that progressed to erosion and ulceration. The wound was swollen and edematous, with extensive loss of skin and subcutaneous tissue along the penile shaft.
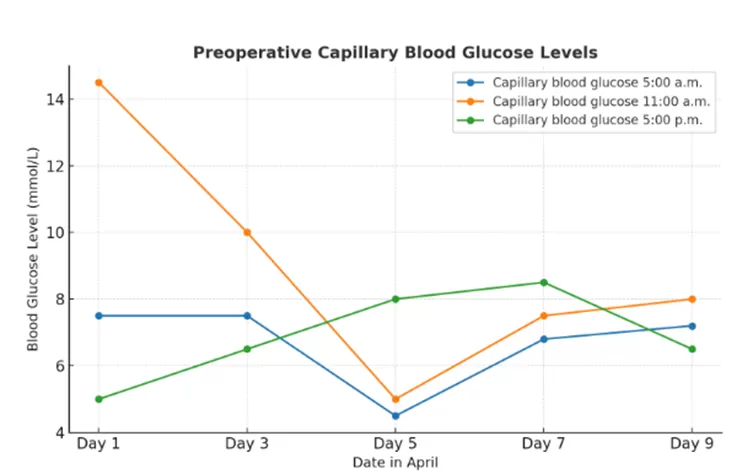
Chart 1. Preoperative blood glucose test results.
Capillary blood glucose measured at 11:00 a.m. showed a significant decrease from an initially high level, reaching its lowest point on day 5 before slightly increasing thereafter. In comparison, glucose levels measured at 5:00 a.m. remained stable until day 3, dropped markedly on day 5, and then gradually rose. Conversely, blood glucose levels recorded at 5:00 p.m. demonstrated a continuous upward trend, peaking on day 7 before declining on day 9. Overall, after day 5, glucose levels at all three time points exhibited a trend toward stabilization.
On April 11, 2025, the patient underwent surgery.
The surgical team evaluated potential donor sites for penile coverage and ultimately selected the scalp, which presents a low risk of infection, excellent vascularity, and is well-suited for split-thickness skin grafting³–⁵. Broad-spectrum intravenous antibiotics were administered preoperatively. The patient was placed in the supine position, with the genital and scalp regions shaved in preparation for surgery.
Surgical technique:
After shaving the designated donor area, the scalp was disinfected, and both general anesthesia and local infiltration anesthesia were administered. Once adequate anesthesia was achieved, a dermatome was used to harvest split-thickness skin grafts sized to match the extent of penile skin loss. The harvested grafts were immediately placed into a sterile bowl containing antibiotic solution. Hemostasis was meticulously achieved at the donor site.
At the recipient site, all necrotic tissue was thoroughly debrided, followed by irrigation with sterile saline and careful hemostasis. The grafts were then positioned over the penile shaft and secured using interrupted sutures with appropriate tension. A bolster dressing and gentle elastic compression bandage were applied to ensure graft adherence and immobilization.
In this case, the graft was fixed with interrupted sutures along its margins combined with light compression, ensuring intimate contact between the graft and the wound bed. This approach minimizes dead space formation and reduces the risk of hematoma or seroma—known factors associated with graft failure. Sutured fixation remains the standard technique for maintaining graft stability in areas subject to frequent movement.

Figure 2. Donor scalp site after skin harvesting.
Regarding the scrotal region, the patient had complete loss of scrotal skin, making direct scrotal grafting infeasible. After careful evaluation of reproductive factors and potential complications, bilateral groin and upper thigh flaps were utilized to reconstruct new scrotal pouches for testicular placement. Each testis was secured within its newly created compartment to minimize the risk of Goldflam reflex or testicular necrosis.
This approach required precise surgical handling to ensure adequate vascularization and minimize postoperative complications while preserving physiological and cosmetic outcomes. The procedure is considered technically demanding because it must balance functional restoration with aesthetic reconstruction in an area of complex anatomy and high infection risk.
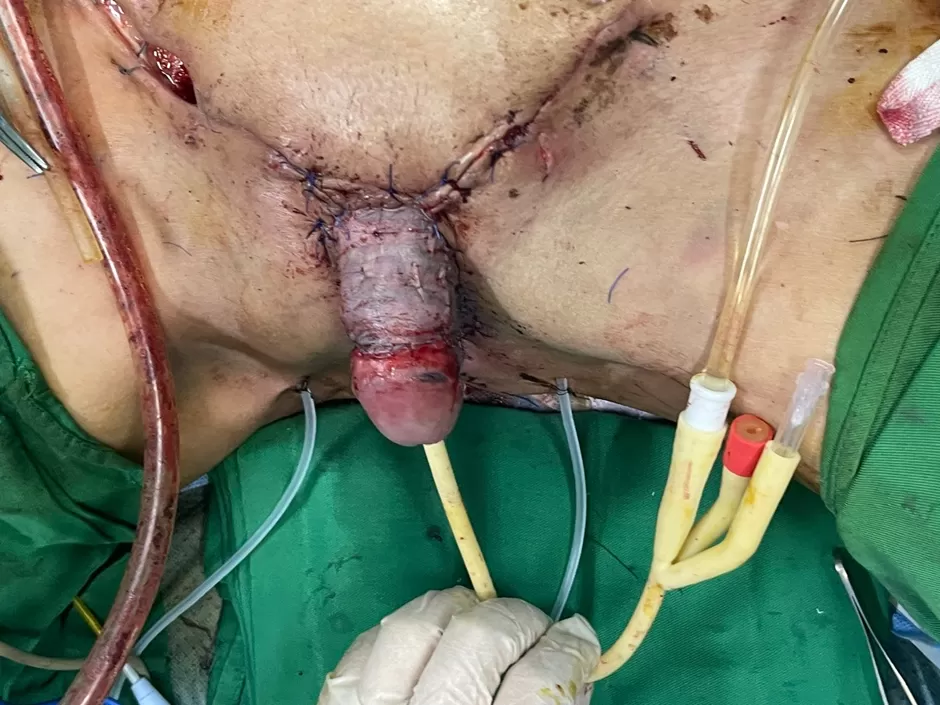
Figure 3. Postoperative view showing the reconstructed penile shaft and inguinal pockets created for testicular placement.
After surgery, the patient was closely monitored in the ward. The surgical wounds remained dry, with no evidence of bleeding or discharge, and both the grafted and flap tissues appeared viable. A urinary drainage catheter was maintained to ensure adequate bladder emptying and to minimize tension on the operative site. Urinary and genital functions were preserved, and no vascular, neural, or testicular injury was observed. The patient’s general condition remained stable, with vital signs within normal limits. He tolerated oral intake, ambulated independently, and showed no postoperative complications.

Figure 4. Daily plasma irradiation applied to the penile graft site.
The patient received daily plasma irradiation therapy to promote wound healing and reduce the risk of postoperative infection. On April 23, the urinary catheter was removed, and the patient was able to void spontaneously without dysuria or discomfort. By April 28, 2025, he was discharged in good general condition—fully conscious and communicative, with a soft, non-tender abdomen, well-healed abdominal incision, and a clean, well-adhered skin graft over the penile and scrotal regions.

Figure 5. Appearance of the penis three months after surgery.
At the three-month follow-up, the patient was in stable general condition, alert, and communicative. Blood glucose was well controlled at 7.8 mmol/L, indicating improved diabetic management compared with the preoperative period. Local examination showed the penile shaft covered with scalp-derived split-thickness skin graft that had healed with stable scarring, a smooth surface, and coloration closely matching the surrounding tissue. No swelling, discharge, contracture, or necrosis was observed, and the graft margins were well defined. Hair growth had resumed over the pubic region, partially covering the penile base and enhancing cosmetic appearance. The abdominal and bilateral inguinal incisions were well healed with soft, non-inflamed scars. The testes, positioned within the inguinal pouches as planned, showed no swelling, tenderness, or abnormalities. The patient reported normal, painless urination, resumed normal personal activities, and demonstrated markedly improved psychological well-being. These outcomes highlight the functional and aesthetic effectiveness of scalp split-thickness skin grafting for penile shaft reconstruction.

Figure 6. Scalp donor site three months after graft harvesting.
The scalp donor site healed rapidly, with complete re-epithelialization and full hair regrowth over the previously harvested area. No visible scarring or residual defect was observed.
Discussion
Diabetes mellitus is a chronic disease associated with numerous severe complications, among which soft tissue infections tend to progress rapidly and are difficult to control⁶. The combination of prolonged hyperglycemia and microvascular damage through glycation processes leads to the formation of advanced glycation end products, which increase collagen stiffness, reduce skin elasticity, and impair wound healing capacity⁷˒⁸. Diabetic patients have a significantly higher rate of surgical site infections and wound dehiscence compared with non-diabetic individuals.
Penile skin loss severely affects sexual, urinary, and psychological functions, posing a major challenge in selecting an optimal reconstructive approach to restore both form and function.
In our case, the patient had type II diabetes mellitus for approximately 6–7 years with poor glycemic control, resulting in immune dysfunction, microcirculatory impairment, and progressive skin tissue damage—all of which increased the risk of necrosis and widespread infection⁵. Given these comorbid conditions, scalp skin was selected as the donor site because of its rich vascularity, rapid healing, and relative resistance to diabetic microangiopathy and infection compared with other regions. These properties enhance graft adherence and reduce infection-related graft failure, while allowing hair regrowth at the donor site³–⁵.
For scrotal reconstruction, several grafting options were considered. However, due to the patient’s advanced age and absence of reproductive demand, bilateral groin flaps were used to reconstruct the scrotum and create subcutaneous pouches for the testes. The use of thick groin flaps elevates local temperature by approximately 2–4°C, which can negatively impact spermatogenesis and sperm quality⁹˒¹⁰. Ahmed and Mbibu also reported using thick skin flaps to transpose the testes into the thigh region for protection¹¹. Similarly, a Chinese study following two patients who underwent scrotal reconstruction using skin flaps demonstrated that this technique poses potential risks to spermatogenesis. Although the reconstruction itself does not physically obstruct spermatogenesis, spermatogenic activity gradually ceases over time. Experimental results in rabbits showed a marked decrease in sperm count, leading to infertility within two months after scrotal reconstruction¹¹,¹².
At three months postoperatively, the patient showed favorable psychological and functional improvement, with satisfactory urinary control. The penile graft site exhibited stable healing, uniform color, and no evidence of necrosis or recurrent infection—an encouraging outcome considering the patient’s long-standing diabetes, which typically delays wound healing and increases infection risk. The use of scalp-derived split-thickness grafts proved highly effective due to the scalp’s rich vascular network, thin and flexible texture, and rapid regrowth of hair at the donor site3,4,5.
Reported skin graft survival rates in diabetic patients range from 70% to 85%, depending on anatomical location and glycemic control¹³˒¹⁴. Nevertheless, it should be noted that scalp skin differs in color and texture from the native penile and scrotal skin, which may influence aesthetic and sensory outcomes. Long-term follow-up is therefore necessary to assess parameters such as tactile sensitivity, elasticity, sexual function, and risk of reinfection. This case also underscores the critical importance of strict glycemic control and meticulous postoperative wound care to optimize reconstructive outcomes in diabetic patients.
Conclusion
After three months, the graft demonstrated complete healing with stable urinary function and no evidence of infection or necrosis, accompanied by improved glycemic control. This technique proved to be both feasible and effective for penile shaft skin reconstruction, particularly in cases where conventional donor sites are unavailable or unsuitable. The use of thick skin flaps or testicular burial for scrotal reconstruction is not recommended in patients who wish to preserve fertility.
REFERENCES
1. Vindenes H. [Skin transplantation]. Tidsskr Nor Laegeforen. 1999;119(27):4050-4053.
2. Simona Federica Spampinato, Grazia Ilaria Caruso, Rocco De Pasquale, Maria Angela Sortino, Sara Merlo. The Treatment of Impaired Wound Healing in Diabetes: Looking among Old Drugs (2020). Pharmaceuticals (Basel). 2020;13(4):60.
3. Dorota Teresa Roodbergen, Adrianus Fredericus Petrus Maria Vloemans, Zjir Mezjda Rashaan, Jacob Cornelis Broertjes, Roelf Simon Breederveld. The scalp as a donor site for skin grafting in burns: retrospective study on complications. Burns Trauma. 2016;4:20. doi:10.1186/s41038-016-0042-z
4. Mimoun M, Chaouat M, Picovski D, Serroussi D, Smarrito S. The scalp is an advantageous donor site for thin-skin grafts: a report on 945 harvested samples. Plast Reconstr Surg. 2006;118(2):369-373. doi:10.1097/01.prs.0000227739.23850.4a
5. Gerhard H. Weyandt, Boris Bauer, Nikolaus Berens, Henning Hamm, Eva-B. Broecker. Split-skin grafting from the scalp: the hidden advantage. Dermatol Surg. 2009;35(12):1873-1879. doi:10.1111/j.1524-4725.2009.01308.x
6. The Immune-Centric Revolution in the Diabetic Foot: Monocytes and Lymphocytes Role in Wound Healing and Tissue Regeneration—A Narrative Review.
7. Nina Dasari, Austin Jiang, Anna Skochdopole, et al. Updates in Diabetic Wound Healing, Inflammation, and Scarring. Semin Plast Surg. 2021;35(3):153-158. doi:10.1055/s-0041-1731460
8. Heather A. Wallace, Brandon M. Basehore, Patrick M. Zito. Wound Healing Phases. In: StatPearls. StatPearls Publishing; 2025. Accessed August 12, 2025. http://www.ncbi.nlm.nih.gov/books/NBK470443/
9. Areej Jorban, Eitan Lunenfeld, Mahmoud Huleihel. Effect of Temperature on the Development of Stages of Spermatogenesis and the Functionality of Sertoli Cells In Vitro. Int J Mol Sci. 2024;25(4):2160. doi:10.3390/ijms25042160
10. Yuanyuan Gao, Chen Wang, Kaixian Wang, Chaofan He, Ke Hu, Meng Liang. The effects and molecular mechanism of heat stress on spermatogenesis and the mitigation measures. Syst Biol Reprod Med. 2022;68(5-6):331-347. doi:10.1080/19396368.2022.2074325
11. Ahmed A, Mbibu NH. Aetiology and management of injuries to male external genitalia in Nigeria. Injury. 2008;39(1):128-133. doi:10.1016/j.injury.2007.02.039
12. Wang D li, Wang Y ming, Zheng H, et al. [An experiment study and clinical observation of the testicle spermatogenesis after scrotum reconstruction]. Zhonghua Zheng Xing Wai Ke Za Zhi. 2004;20(3):203-205.
13. “Outcomes of Skin Graft Take After Use of VAC in Duabetic Patients” by Abdelrazek A. G. Hassan, Abdelaziz A. Taalab et al. Accessed August 12, 2025. https://www.menoufia-med-j.com/journal/vol38/iss2/31/?utm_source=
14. Lamani YP, Reddy MA, Kalburgi EB, Suhas BS. Comparison of split skin thickness graft survival in diabetic and non-diabetic ulcer. International Surgery Journal. 2020;7(4):1238-1242. doi:10.18203/2349-2902.isj20201404
Nguồn: Phòng NCKH&CN